The Window of Tolerance for Trauma: A Practical Guide to Understanding Your Nervous System

If you’ve ever swung between feeling completely overwhelmed and feeling nothing at all, you already know what it’s like to live outside your window of tolerance. You may not have had a name for it. But the experiences — the anxiety that won’t settle, the numbness that won’t lift, the sense that your reactions are bigger or flatter than the situation warrants — is something many people healing from trauma know intimately.
Understanding your window of tolerance for trauma won’t resolve that on its own. But it gives you something you may not have had before: a way to know where you are, what your nervous system actually needs in that moment, and whether what’s happening inside you is a response to a real, present threat — or an echo of something older.
That distinction matters more than most nervous system content acknowledges. This article is about why.
What the window of tolerance actually is
The window of tolerance is a concept introduced by psychiatrist Dan Siegel in 1999. It describes a zone of nervous system activation where you can function, where you can feel your emotions, think clearly, make choices, and engage with other people. Inside that window, you can handle stress without being consumed by it.
Outside it, things get harder. Your access to conscious reasoning narrows. Your responses become more automatic, more driven by what kept you safe before than by what you actually want to do now. You may behave in ways you don’t recognize or don’t like and then blame yourself for them, without understanding that they weren’t really choices.
The window isn’t fixed. It expands and contracts depending on what has happened to you, what’s happening now, and how much capacity your nervous system has built, which, for most trauma survivors, was never given the conditions to develop fully. People who grew up in environments that were unsafe, unpredictable, or emotionally dismissive often enter adulthood with a narrow window. Not because something is wrong with them, but because their nervous system adapted to what it had to work with. The goal isn’t to stay in your window of tolerance at all times. That’s not possible, and it’s not the point. The point is to know when you’ve left it and what to do next.
The window of tolerance is a useful framework for understanding your nervous system in trauma recovery. It’s also not enough to heal trauma on its own and I want to be clear about that from the start. What it gives you is a map of where you are and what your nervous system needs in a given moment. What to do with that, the deeper work of healing, is a longer conversation.
Prefer to listen? Here’s the episode Window of Tolerance for Trauma:
Dysregulation isn’t just “off” — it has a direction.
This is where most window of tolerance explanations stop being useful.
When we talk about being dysregulated, we tend to treat it as a single state, whether it’s out of balance, overwhelmed, not okay. But dysregulation has a direction, and that direction determines everything about what your nervous system actually needs.
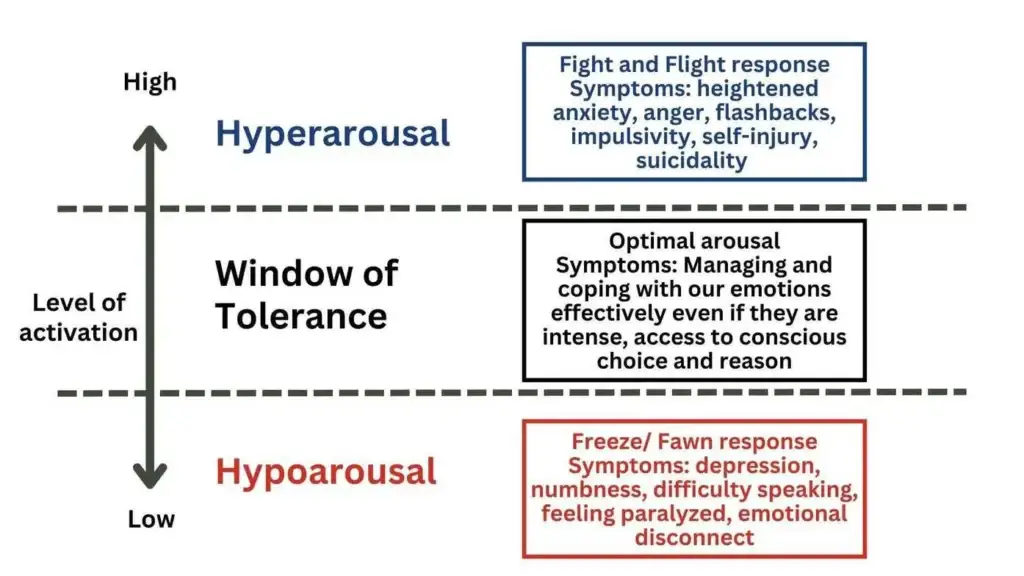
Hyperarousal is dysregulation upward, past the upper boundary of your window. Your nervous system is overactivated. You may feel anxious, agitated, or on edge. Thoughts race. Muscles tighten. Anger rises fast. Sleep becomes difficult. In more intense states, you may experience flashbacks, panic, or a sense of being out of control. This is the fight-or-flight response, your nervous system mobilizing energy to meet a perceived threat.
Hypoarousal is dysregulation downward, past the lower boundary. Your nervous system shifts into shutdown. You may feel numb, foggy, or disconnected from your body or emotions. Depression can settle in. Motivation disappears. Speaking or thinking clearly feels effortful. This is a shut down response where your nervous system conserving resources or going still in the face of a threat it couldn’t fight or flee.
Many people live primarily in one of these states. Others cycle between them, activated and then collapsed, overwhelmed and then shut down. Both are adaptive responses to extreme circumstances. Both are your nervous system trying to protect you. And they require opposite interventions.
If you’re in hyperarousal, your nervous system needs to be calmed, brought down from high activation into a more regulated state.
If you’re in hypoarousal, your nervous system needs to be stimulated, gently activated out of shutdown and back toward engagement.
Applying a calming strategy when you’re numb or frozen, or a stimulating one when you’re already flooded, doesn’t just fail to help. It can make things worse. Knowing which direction you’re dysregulated in is the first practical step.
Emotions can push you out of your window, too.
Dysregulation doesn’t only come from external events. Certain emotions, particularly the ones that carry the most charge in your history, can push you out of your window of tolerance on their own.
Shame is the most common one. For many people who have experienced trauma, especially childhood trauma or complex trauma, shame doesn’t just feel bad — it’s activating in a way that collapses the window almost immediately. Grief can do this. Rage can do this. Emotional pain or abandonment can do it. Emotions that were never safe to feel, never witnessed, never moved through, they don’t disappear. They live in our bodies and get reactivated, sometimes by circumstances that seem disproportionate to the response they produce.
When you find yourself dysregulated and can’t identify an obvious external trigger, this is worth considering. Something internal moved. A memory, a feeling, a part of you that carries an old wound and was touched by something in the present moment.
What activated it — and is the threat actually real?
One of the most important questions you can learn to ask when you notice you’re dysregulated is: what activated this, and is it a real, present threat?
This isn’t about dismissing your response. Your nervous system’s reaction is always real. The question is whether it’s responding to what’s happening now, or to something from the past that the present moment resembles closely enough to trigger the same alarm, or both.
Trauma leaves imprints. A tone of voice, a particular silence, a smell, a look on someone’s face, any of these can activate a nervous system that learned, in an earlier time, that these things meant danger. The activation feels identical to what it felt like then. The body doesn’t automatically know the difference between then and now.
Learning to pause and ask: Is there an actual threat here, or is my nervous system responding to something it recognizes from before, or maybe both? is harder than it sounds. But the practice of asking builds something: a part of you that can observe your state without being consumed by it. Listen to: Understanding childhood trauma triggers in adulthood.
Awareness as the foundation of early trauma recovery
In my work with clients, building this awareness is central to the first stage of trauma recovery, before we move into processing traumatic memories or before we go deeper into parts work or EMDR.
If you don’t know when you’re dysregulated, or which direction you’re in, or what tends to activate it, you can’t intervene effectively. You’re reacting without information. And that’s exhausting, not because you’re doing something wrong, but because you’re navigating without a map.
Dysregulation can feel crazymaking. It activates parts that carry shame, parts that have strong opinions about what it means that you’re not okay. But dysregulation itself is just a nervous system state. It’s not evidence of how broken you are. It’s information about where you are right now.
Many people start trauma recovery afraid of what might happen if they open the box — what they’ll find, whether they’ll be able to handle it. That fear is natural. Learning to work with your window of tolerance for trauma recovery gives something back: a sense that you have tools, that you can recognize when you’re overwhelmed, that you can return to a more regulated state. It doesn’t eliminate the fear. But it makes moving forward feel less like stepping off a cliff.
What I teach clients first is this: check in. Where am I right now? What state is my nervous system in? What does it feel like in my body? What might have shifted me here?
In session, when a client starts to feel outside their window, I’ll ask: What’s the intensity right now on a scale of zero to ten? Sometimes it’s a five. Sometimes an eight. Then I ask whether they want a grounding practice. The threshold is theirs, not mine. Some clients don’t want to go above a six. Others can stay with an eight but not a nine. We work with what they tell me.
Early in trauma recovery, this matters for a specific reason — not just so you can cope, but so we don’t push past what your system can handle. Most people carry strong “push through” parts. They’ve survived by overriding their own signals for years. Learning to notice the signal before overriding it is new territory.
That’s also how the window expands. Not by pushing through, but by staying — being with a five long enough that it becomes familiar, until a six is possible. Over time, what was intolerable becomes something the nervous system can hold. Your states become information rather than emergencies. That’s a different way of being with yourself than most trauma survivors have ever had.
Strategies — organized by what your nervous system actually needs
Once you can identify your state and its direction, you can choose an intervention that fits.
If you’re in hyperarousal: calming your nervous system
The goal is to reduce the activation.
Breathwork. Slow, deliberate breathing, particularly extending the exhale, activates the parasympathetic nervous system and begins to reduce arousal. Start by simply noticing your breath without trying to change it. Then experiment with directing the breath into your belly rather than your chest. The shift may be subtle at first. That’s normal. If breathing is hard to access, put your hand on your heart or any other place in your body where you feel sensation, and sigh it out.
5-4-3-2-1 grounding. This is probably the most widely used grounding practice in trauma work, and one of the easiest to access. Name five things you can see, four you can hear, three you can physically feel, two you can smell, and one you can taste. Say them plainly, without added meaning. The point is contact with the present, not the past, not the feared future. Check your emotional intensity before and after on a scale of 0–10. Even a small shift is meaningful. Personally, I use it most with anxiety. It’s particularly effective when the nervous system is activated rather than shut down.
If tracking your body is activating rather than grounding, stay entirely with sight. Reconnection to our bodies isn’t a process that should be forced, and there’s no ideal standard. What are five things you can see that are blue? Three things that are round? Keep it external until contact with your body feels safer.
Going outside. For some people, the sky, air, and the sensation of wind on their face are regulating. For others, being outside increases anxiety. Know which is true for you.
If you’re in hypoarousal: Stimulating your nervous system
The goal is the opposite — to gently activate a shutdown system.
Physical movement. Jumping jacks, planks, or push-ups, anything that introduces physical activation. Start with whatever is accessible. If jumping jacks feel impossible, walking is enough. If walking feels impossible, standing up and moving around the room is a start. Meet your nervous system where it actually is, not where you think it should be.
Upbeat music or dancing. Rhythm and tempo stimulate your nervous system when stillness keeps you stuck. Dancing adds the physical component. Either works.
A short walk outside. Light physical activation and contact with the external environment at the same time. For many people in hypoarousal, nature restores a sense of connection that shutdown severs.
A note on practice
These tools need to be practiced when you don’t urgently need them. That’s how they become available when you do. In the beginning, if you’re at a very heightened state, they may not work at all. And that’s expected, not failure. Look for 1% improvement, not a shift from zero to a hundred.
Staci Haines once said in a training I attended: we need to embody an experience 300 times before we can use it under regular stress, and 3000 times under high stress. That number didn’t discourage me. It very much aligned with my own experience in trauma recovery. I now often share it with my clients so that they have an idea of what to expect.
I spent several months in sustained hypoarousal after an experience of systemic violence. In the beginning, nothing seemed to move. The shifts were so small I couldn’t detect them week to week. It took reassessing at six months, then a year, to see how much had actually changed. If you have experienced childhood trauma, you are often building several layers at the same time: learning to manage emotions while expanding your window of tolerance for trauma recovery. Your brain’s pathways were shaped by dysregulation. Each time you respond differently, you’re building new ones. It just may take longer than anyone tells you it will. Don’t evaluate too early. And don’t stop.
What this points toward
The window of tolerance for trauma is a starting point, not a destination. Building awareness of your states, understanding what activates them, and developing the capacity to return to your window, this is the foundation that makes deeper trauma work possible.
I want to be direct about something: working with your window of tolerance will not heal childhood trauma or complex trauma. It’s one useful step, an important one, but it’s not enough.
What grounding tools do is create enough stability to begin the deeper work. The parts that carry shame, grief, pain or rage — the ones that push you out of your window in the first place — don’t heal because you learned to breathe through activation. They heal when they’re worked with directly. That’s a different kind of work.
In my practice, I integrate the window of tolerance throughout the Integrative Trauma Recovery Model™, my approach to trauma counselling, alongside parts work and EMDR, not as a preliminary stage you complete and leave behind. Regulation and healing happen together, not in sequence.
Want to dig deeper?
If you have experienced childhood trauma:
Parts work therapy to heal childhood trauma as an adult: What parts actually are, why talk therapy often doesn’t reach them, and what turning toward them looks like in practice.
EMDR for childhood trauma : Why EMDR alone isn’t enough for childhood trauma, what the foundation actually requires, and what becomes possible when it’s done right.
If you have experienced complex trauma:
IFS or EMDR for complex trauma: Why neither approach alone is enough for complex trauma, and what a genuinely integrative approach actually looks like.
Sources
Window of tolerance for trauma draws from the following sources:
Fisher, J. (2023). Janina Fisher’s Trauma treatment certification training (CCTP): The latest proven techniques to resolve deeply held trauma [Online professional training]. PESI
Haines, S. (2022). Safety, belonging, and dignity: Using the generative power of somatics to heal individual and systemic trauma. [Online professional training]. Academy of Therapy Wisdom
Davis, E., & Marchand, J. (2021). Attachment and dissociation assessment and treatment [Online professional training]. R. Cassidey Seminars
Greenwald, R. (2020). EMDR basic training, approved by the EMDR International Association (EMDRIA). [Online professional training]. Trauma Institute & Child Trauma Institute
Vancouver College of Counsellor Training. (2016). Sexual Abuse Counselling Skills [In-person professional training]. Vancouver, BC, Canada.
Disclaimer: This content reflects my professional knowledge and experience and is intended to educate and support. It may not apply to every situation, and I don’t know your specific context. If you feel stuck, notice symptoms that limit your ability to participate in daily life, or experience worsening distress, I encourage you to reach out to a qualified mental health professional for individualized support.
Unsure where to go? Start with:
Healing trauma: What recovery actually requires: the phases, the approaches and why healing isn’t about coping forever.
Healing childhood trauma as an adult: What childhood trauma looks like in adulthood, why the effects don’t just go away, and what healing actually involves — from someone who has lived it.
About Natalie

I’m Natalie Jovanic, a trauma counsellor and complex trauma coach with over 15 years of experience in complex, childhood, and relational trauma. I bring together clinical depth and the embodied experience of full recovery. I developed the Integrative Trauma Recovery Model™ to support more than symptom relief — helping people restore relational health, rebuild self-trust, and reconnect with vitality in their lives. I also host the podcast Trauma Demystified.
If you’re noticing patterns you can’t seem to change, this guide may help you understand why.
About my approach
My writing reflects my training, lived experience, and how I practice. I share what I believe represents best practice in trauma recovery — and I always encourage you to notice what feels right for you.